
Food as medicine interventions increase access to nutritious foods for food-insecure individuals living with diet-related chronic disease.
Food insecurity, the household-level economic and social condition of limited or uncertain access to adequate food, significantly increases the risk of developing or worsening chronic illnesses like diabetes, heart disease, hypertension, and asthma by forcing reliance on inexpensive, nutrient-poor foods, contributing to chronic stress, and disrupting medication use.
“Food-as-medicine” (FAM) refers to a spectrum of evidence-based interventions (Fig. 1) that integrate consistent access to nutritious food into healthcare to directly address the medical nutritional needs of individuals with diet-related medical conditions, including but not limited to those experiencing food insecurity. After being screened for risk factors, eligible individuals are referred to FAM programs by a medical provider. Program services are then offered by an implementing organization, typically at no cost to the participant.
The Food is Medicine Pyramid: An Evolving Set of Healthcare and Population-Health Programs that Integrate Food-Based Nutrition Interventions at Multiple Levels
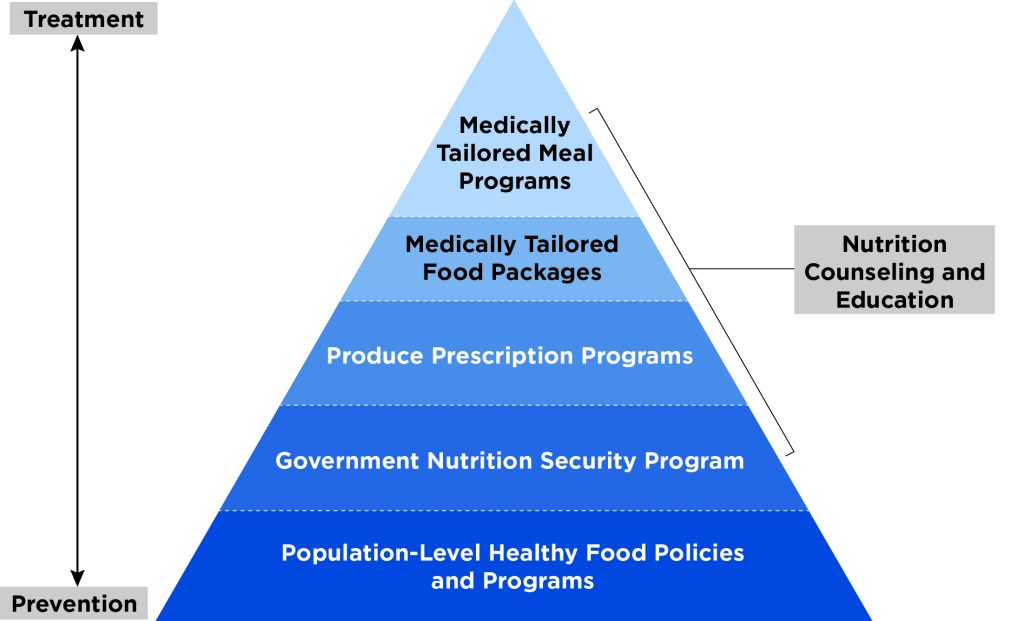
SOURCE: Dariush Mozaffarian et al., “A Food is Medicine approach to achieve nutrition security and improve health,” Nature Medicine 28 (November 2022): 2238–40, https://doi.org/10.1038/s41591-022-02027-3.
There are three primary models of direct FAM interventions. These interventions offer varying levels of customization appropriate for different target populations.
- Medically tailored meals (MTMs) are fully prepared meals designed by Registered Dietitian Nutritionists (RDNs) to meet the dietary needs of individuals with complex or severe medical conditions who face physical limitations in preparing meals.
- Medically tailored groceries (MTGs) are boxes of minimally processed grocery items selected by an RDN that patients use to prepare healthy meals at home. Like MTMs, MTGs are personalized interventions, designed to meet individual medical needs (e.g., low-sodium foods for patients with hypertension).
- Produce prescriptions (PRx) that are written by healthcare providers for individuals who have or are at high risk for diet-related diseases. These prescriptions can be redeemed for fruits and vegetables of the patients’ choice at participating stores or farmers’ markets.
These three FAM interventions are downstream complements to broader policy efforts aimed at improving population-level nutrition security, such as the Supplemental Nutrition Assistance Program (SNAP).
Food-as-medicine interventions reduce food insecurity and improve dietary quality among participants.
FAM programs change the way people eat by addressing financial constraints to consuming healthy food, with research consistently showing decreases in self-reported food insecurity at the end of intervention periods. Participation in FAM programs is also associated with increases in fruit and vegetable intake and small decreases in the consumption of less nutritious foods, bringing patients’ diets into closer alignment with dietary guidelines. The nutrition education included in many FAM interventions also helps address knowledge and culinary barriers to healthy eating, improving the likelihood of long-term adoption of these dietary changes.
Emerging evidence suggests food-as-medicine interventions may improve patient health and reduce long-term healthcare spending, although additional research is needed.
Observational studies, quasi-experimental analyses, and a smaller but expanding number of randomized trials suggest that the dietary changes, reduced stress, and improved disease self-management capacity induced by FAM interventions may be associated with modest improvements in select clinical outcomes, including blood sugar (A1C), LDL cholesterol, and blood pressure. However, results are inconsistent and vary based on intervention design, leading to calls for more large-scale and standardized studies.
Studies also report associations between FAM interventions and reduced hospital admissions, emergency department visits, and overall healthcare expenditures among high-risk populations. These improvements could have widespread economic impacts, with one study estimating that nationwide access to MTMs could yield savings of up to $13.6 billion annually.
The impact of food-as-medicine policies is determined by their design.
The Health Equity Reform amendment to New York’s Medicaid 1115 waiver expands access to FAM interventions, creating Social Care Networks (SCNs) that partner with existing community-based organizations to screen, refer, and provide services to eligible Medicaid members. As of 2024, similar demonstrations were pending or approved in nine other states. While evaluation of these approaches is limited given their novelty, the growing shift from fragmented pilot programs to a systematic, healthcare-integrated model offers tailored support for stakeholders that qualitative research suggests is essential for program success. Stronger policy support for practices such as universal patient screening, expanded staff training, and the use of integrated Electronic Medical Record systems has been suggested to further strengthen program impact.
At an individual level, participation in and efficacy of FAM interventions are affected by the convenience, accessibility, and cultural relevance of services. Trust in providers and concerns about stigma also play a role, suggesting the need for screening tools and service provision locations that minimize patient discomfort. At a food systems level, the economic impacts of FAM programs are shaped by their sourcing strategies. A recent analysis suggests that by keeping healthcare dollars in the state economy, enrolling all eligible patients in FAM programs that purchase from local producers and food businesses whenever possible could create over 18,000 jobs, support 630 small to midsized farms, and result in a potential $2.7 billion increase in New York’s GDP. Collectively, this research highlights that the effects of FAM programs are not fixed, but contingent on a range of program implementation choices.
ABOUT THE AUTHOR(S)
Ashmita Das is a New York State Science Policy fellow at the Rockefeller Institute of Government.